
The Surgery That Learned to Stop Cutting
Breast Augmentation: a new system might be a step forward. The evidence is still catching up.


The Plane Problem
The breast sits over the pectoralis major muscle. For decades, surgeons had two choices for placing an implant: in front of the muscle, or behind it. Each choice was a trade.
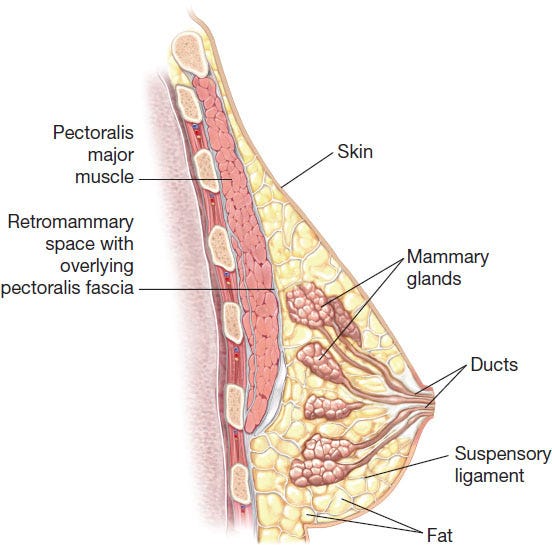
Go in front — the subglandular plane — and the surgery was simple, recovery fast, and muscle untouched. But capsular contracture rates were high, up to 38% with smooth implants in some studies.
Go behind the muscle — subpectoral — and contracture rates dropped. Coverage improved. But the pectoralis movement can cause the implant to jump when the muscle flexes. This is called animation deformity.
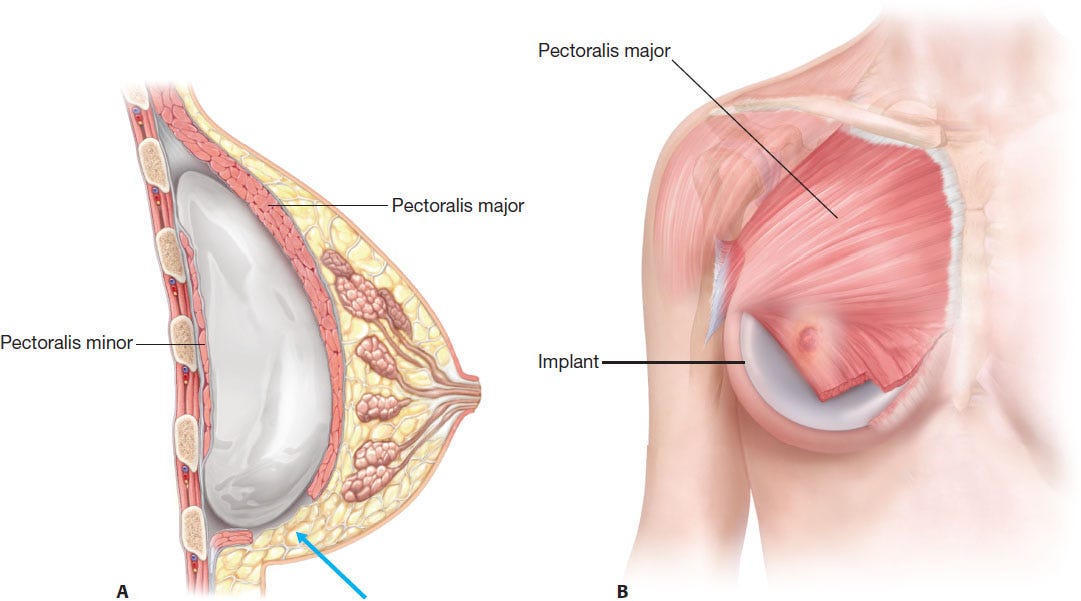
Tebbetts formalized the dual plane technique in 2001. Partial release, variable coverage, a spectrum of subtypes. It was elegant and it helped. Contracture came down. But the muscle still fired. Pain at recovery was still significant. The tradeoff had been refined, not resolved.
The Fascial Option
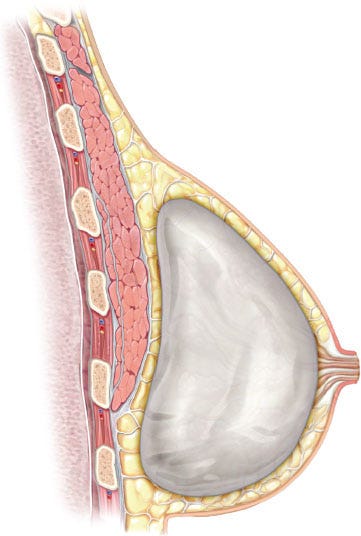
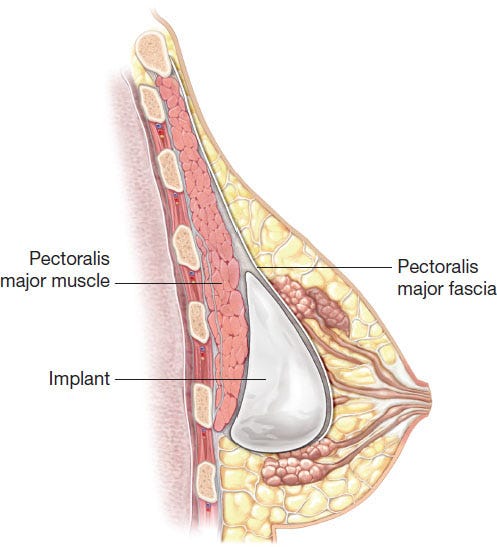
The subfascial plane was described in 2003. Place the implant beneath the thin collagenous fascia covering the muscle — above the muscle fibers, below the gland. No muscle release. No animation deformity. A biological barrier between implant and breast ducts. This appeared to reduce contracture.
The data came in slowly but it held. A systematic meta-analysis pooled subfascial contracture rates at roughly 1%. Hematoma and seroma rates were lower than subglandular. Implant malposition was better. Lateral malposition in one direct comparison ran 8.8% subfascial against 23.4% for the dual plane group. The double bubble deformity appeared in zero subfascial patients and 3.7% of subpectoral patients.
The Preservation Argument
That is where a Costa Rican surgeon and a medical device company saw an opportunity. Establishment Labs designed a new system, called Preservé. Whether it represents a genuine paradigm shift or an incremental improvement with good marketing is, at this point, an open question.

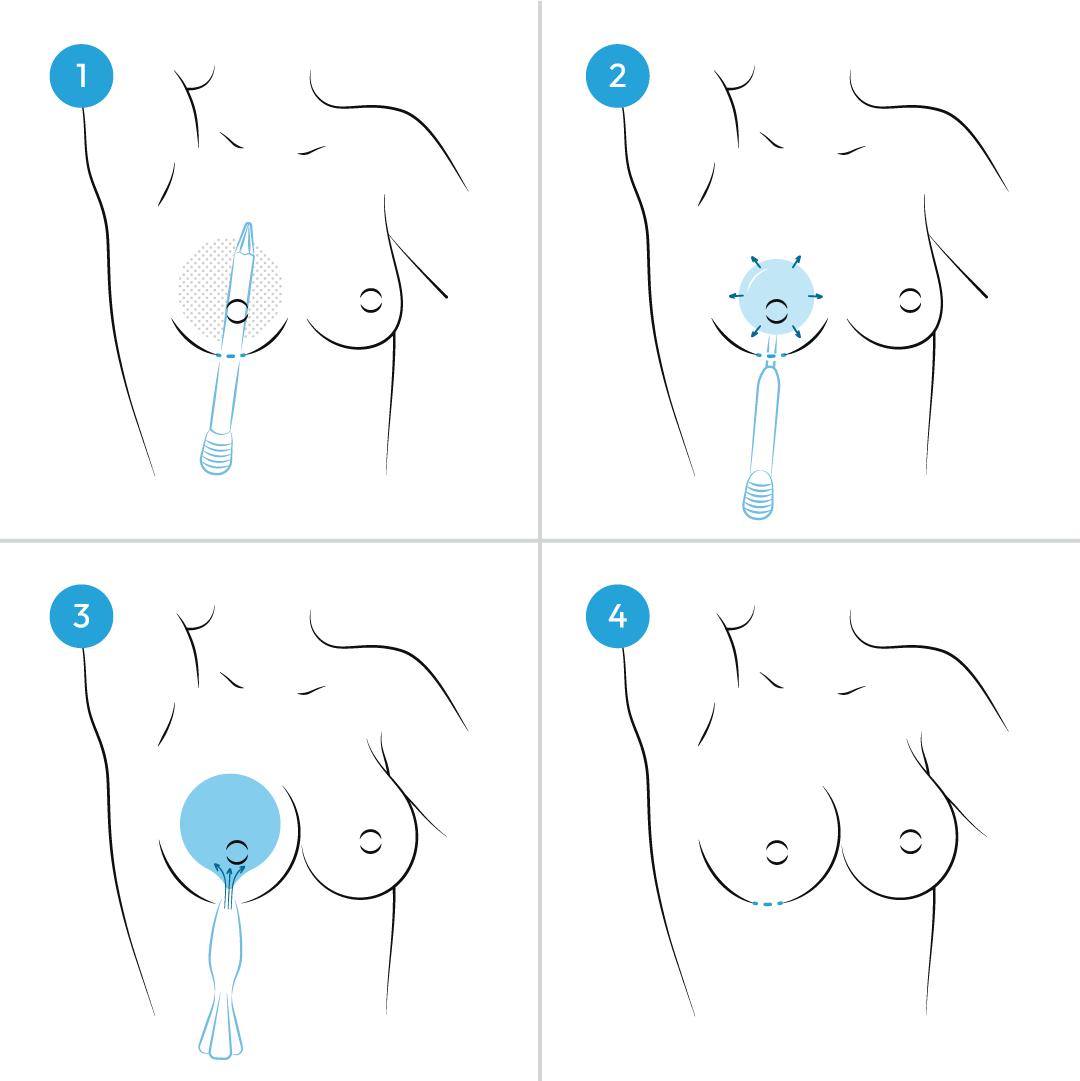
The pitch is straightforward: create the pocket by expanding tissue rather than cutting through it. In the prepectoral space, an inflatable balloon is advanced and expanded slowly, distributing pressure evenly to lift the breast away from the pectoralis muscle. The claim is that this pushes aside the breast’s tissue rather than injuring it. Then the implant goes in using a no-touch funnel. Whether the tissues remember the difference is the question the long-term data will eventually answer.
The feasibility study showed 0% inferior malposition at three years — a striking number from a small, industry-sponsored study using an implant not yet FDA-approved. The broader study showed capsular contracture at 0.5% and rupture at 0.6% at five years. Genuinely low. Also a single-arm study with no control group. The ten-year data is not in yet, and the outcome numbers cited in promotional materials were generated with a different implant in other countries. The no-touch delivery reduces one known contamination pathway. The rest is mostly theory awaiting longer data.
The mechanism makes biological sense. The evidence does not yet match the confidence of the pitch.
What It Means
Breast augmentation has spent sixty years negotiating between coverage and consequence. The subglandular plane caused hardening (higher risk of capsular contracture). The submuscular plane caused distortion (higher risk of animation deformity). The subfascial plane reduced both – a sweet spot – but took two decades to prove it. Each advance looked promising early and required time to earn its place.
Preservé arrives with a sound concept and encouraging early numbers. The history of this field is a long lesson in the distance between the two. It deserves a serious look. It does not yet deserve a verdict.